
Jesus Wept: How Trump, RFK Jr., and Religion will Kill Children
Trump, RFK Jr., and Dr. Kirk Milhoan did not stumble into a public health catastrophe. They built one for reasons that had nothing to do with children and everything to do with themselves

Start with a number. In 1952, the United States recorded 57,628 cases of poliomyelitis. Thousands were paralyzed. More than three thousand died. In hospitals across the country, children lay inside iron lungs, large metal cylinders that mechanically expanded the chest cavity because the patients could no longer breathe on their own. Some of those children stayed in them for months. Some for years. Jonas Salk’s inactivated vaccine, declared safe and effective in April 1955, changed all of that. By 1979, wild poliovirus had been eliminated from the United States entirely. The vaccine worked. Its safety profile, established across hundreds of millions of doses over seven decades of continuous surveillance, is not a subject of legitimate scientific dispute. And yet, in January 2026, the man now chairing the federal committee that sets the American childhood.
His name is Kirk Milhoan. He is a pediatric cardiologist, a former Air Force flight surgeon with two combat tours in Iraq, and an ordained evangelical Christian pastor at Calvary Chapel South Maui in Hawaii. His wife has described his callings publicly as doctor, soldier, pastor, missionary, and he appears to take all four with equal seriousness. He also, based on the public record, does not understand basic polio epidemiology, has compared pandemic vaccine mandates to the Holocaust, told a Texas church congregation that mRNA technology is the biggest threat to humanity, and claimed without any scientific basis that receiving a COVID vaccine in the first trimester of pregnancy carried an 80 percent chance of miscarriage. In June 2025, Robert F. Kennedy Jr. fired all 17 existing members of the Advisory Committee on Immunization Practices and replaced them, with one exception, with people who are either anti-vaccine activists or lack relevant expertise. Then Kennedy made Milhoan their chair.
To understand why that matters, you need to understand what ACIP actually does, because the name sounds procedural and the function is anything but. ACIP is the CDC panel responsible for determining the United States childhood vaccine schedule. It does not approve vaccines. What it does is arguably more consequential: it decides which vaccines are recommended for routine use, and under the Affordable Care Act, any vaccine that receives a Category A recommendation from ACIP must be covered by private insurers at no cost to the patient. Medicare and Medicaid follow the same guidance. When ACIP recommends a vaccine, it becomes accessible to virtually every child in America regardless of their family’s income. When ACIP quietly delays, weakens, or removes a recommendation, that coverage disappears. The vaccine does not become illegal. It becomes something a family has to pay for out of pocket, which for tens of millions of Americans is the functional equivalent of unavailable.
The committee Milhoan now chairs has already reduced the number of recommended childhood vaccines from 17 to 11. It voted to eliminate the universal birth-dose recommendation for hepatitis B, a vaccine that prevents perinatal transmission from mothers who may not know they are infected. Public health officials described that decision as a predictable death sentence for a calculable number of infants. These are not abstractions. They are policy choices with specific, measurable downstream mortality attached to them.
Milhoan’s January 2026 podcast interview is worth examining in some detail, because it reveals something important about how he thinks, or more precisely, about what he has substituted for thinking. When asked whether vaccines have been appropriately studied for safety, he said: No. They haven’t been. They’ve only been studied for efficacy. This is false in a way that should disqualify a person from the position he holds. Before licensure in the United States, vaccines must complete Phase I, II, and III clinical trials evaluating both safety and efficacy. Phase III trials typically enroll tens of thousands of participants and are specifically designed to detect adverse events. After licensure, vaccines enter a multi-layered post-market surveillance system: the Vaccine Adverse Event Reporting System, the Vaccine Safety Datalink, a collaboration between the CDC and nine large health systems covering approximately 12 million patients, and the Clinical Immunization Safety Assessment Project. The VSD alone carries the statistical power to detect adverse events occurring at rates as low as one per million doses. This is one of the most comprehensive pharmacovigilance architectures in the world. Milhoan either does not know this, in which case he is unqualified, or he knows it and chose to say otherwise, in which case he is something worse.
When a podcast host noted that ACIP would be reviewing data based on established science, Milhoan replied: That’s not science. Dr. Paul Offit, a pediatric infectious disease specialist at Children’s Hospital of Philadelphia and one of the most respected vaccine researchers in the country, called the interview frightening and said Milhoan’s comments were directly averse to the health of children in this country. Offit also noted that when Milhoan questioned whether the country still needs the polio vaccine, citing improved sanitation as a reason, he had the epidemiology precisely backwards. In low-sanitation environments, infants encounter poliovirus early in life while still carrying maternal antibodies, which typically produces mild or asymptomatic infection and confers natural immunity. As sanitation improved in the twentieth century, exposure was delayed until after maternal antibodies had waned. Children encountered the virus older and unprotected, and paralytic outcomes increased. This is why the 1952 American epidemic was so catastrophic: the United States was a wealthy, high-sanitation country, and that made it more vulnerable, not less. Offit put it plainly. A lot of people don’t know that, he said. But what upsets me is that he’s in a position where he should know it.
Milhoan’s record before he was appointed chair makes the appointment harder to explain as an oversight. During the COVID pandemic, he did not require masks or social distancing at his church, saying the mission had to continue. He treated patients with ivermectin and hydroxychloroquine after randomized controlled trials had established their inefficacy against COVID. His conduct drew public condemnation from Hawaii’s governor and state health director. His medical license was placed under review. In October 2025, he told a Texas church congregation that COVID was a bioterror weapon. He lost his position at his pediatric cardiology practice. His wife attributed the firing publicly to an overwhelming number of calls demanding his removal. Shortly after an ACIP meeting in December 2025, he was overheard comparing fellow committee members to puppets on a string. He remains the chair of ACIP.
In his podcast interview, Milhoan described his decision-making standard this way: My higher authority for me is I stand before God, and if I harm children by action or inaction, both of those are critical to me. It is worth reading that carefully. He is not describing a scientific standard. He is not describing an epidemiological framework or a methodology for weighing population-level risk. He is describing a theological one. And when the man running the panel that determines what vaccines 80 million Americans’ insurance plans are legally required to cover tells you that his higher authority is God rather than evidence, he is not being humble. He is telling you that no accumulation of data can change his conclusions, because his conclusions were not derived from data. They were derived from faith. Faith, by design, is not falsifiable. That is precisely what makes it unsuitable as the operating principle of a public health committee.
Milhoan is in that chair because of Robert F. Kennedy Jr., who is in his position because of Donald Trump. Understanding how that chain was constructed requires setting aside the idea that any of it was accidental.

Start with Kennedy. After a heroin arrest, his options collapsed — politics off the table, law firms uninterested, a DA’s office out of the question. What he could land was a volunteer slot with Riverkeeper, a nonprofit cleaning up the Hudson, something he picked up during probation. He leveraged it into decades of environmental work, a law clinic, a family-name-polished reputation as a crusader. It looked like reinvention. His former colleagues at the Natural Resources Defense Council, where he spent nearly thirty years, have a different read. Robert Hartl, who grew up on the Hudson and worked alongside him, isn’t confused about the timeline. “RFK has been twisted for decades,” he told HuffPost. “Nothing is new, people just tolerated his untethered and bizarre beliefs because his last name was Kennedy.” He called him “an environmental criminal and an environmental villain.” Dan Reicher, a Stanford energy researcher who worked with Kennedy at the NRDC and kayaked with him on multiple continents, was more concise: “Stay very far away from today’s RFK Jr. if you’re interested in environmental protection.”
One of the myths Kennedy needed to sell was the fiction of being the brave outsider — and as a Kennedy, that's a substantial lift. His name alone opened every door his heroin arrest tried to close. The outsider pose required ignoring that, required the audience to ignore it too, and the longer it ran, the more the fiction mattered more than the facts. That's the tell. When the evidence stopped cooperating, Kennedy stopped following the evidence.
His organization, Children’s Health Defense, has been identified as one of twelve accounts responsible for the majority of anti-vaccine misinformation on major social media platforms. The autism-vaccine claim he’s promoted for years traces to a single 1998 Lancet paper — retracted in 2010, data fabricated, author paid by lawyers suing vaccine manufacturers, author subsequently stripped of his medical license. Kennedy has known this for years. He has continued anyway.*
Courage isn’t what this is. It’s cruelty dressed as courage — and the costume has to be maintained. Audiences don’t sustain themselves. Keeping them meant Kennedy had to keep lying, about things he had every reason to know were lies, to people who trusted him with their children’s health.
Trump is the simplest case of the three, though simplicity should not be confused with a lesser degree of culpability. He does not read epidemiological literature. He does not convene experts and weigh competing evidence in good faith. He identifies constituencies and performs for them. When a politically available bloc of vaccine skeptics materialized after COVID, organized and furious at every institution that had told them what to do, Trump recognized not a public health concern but a voting opportunity. Kennedy had a famous name, a cultivated outsider image, and a demonstrated ability to mobilize distrust of mainstream medicine. Trump did not need to believe a word of it. He needed Kennedy’s voters. The appointment was transactional in a way that was not even particularly concealed. The cost of that transaction is being paid by children who will contract preventable diseases, by infants too young to be vaccinated who will be exposed by older unvaccinated children in their communities, and by immunocompromised Americans who depend on herd immunity because they cannot protect themselves.
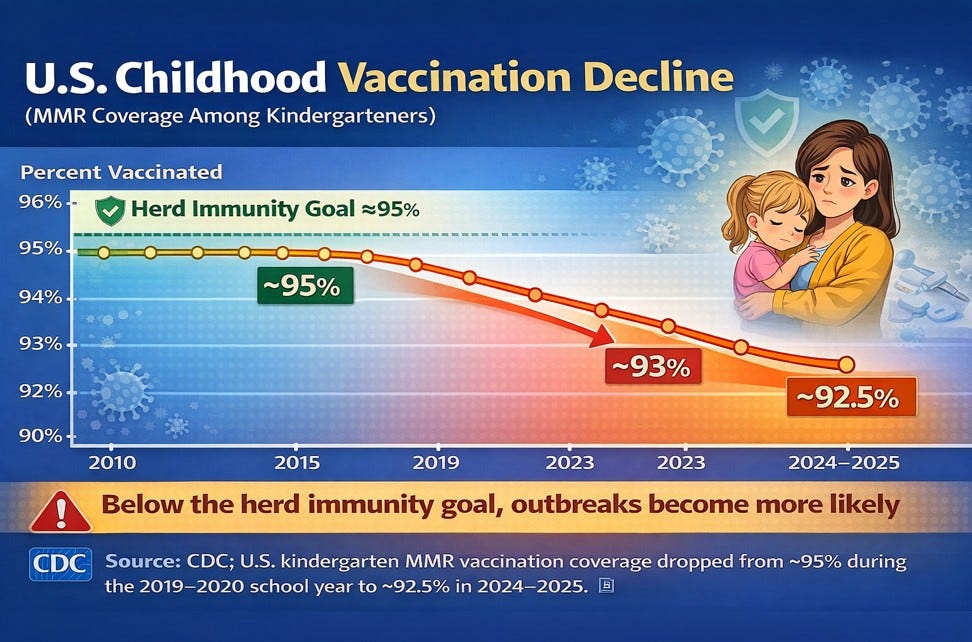
Herd immunity is not a courtesy. It is a mathematical threshold built from the accumulated vaccination decisions of millions of people, a firewall that protects those who biologically cannot protect themselves: newborns, patients in chemotherapy, transplant recipients on immunosuppressants, people with primary immunodeficiency disorders. For measles, that threshold sits at roughly 95 percent vaccination coverage. Drop below it and the virus finds its opening. When ACIP removes a Category A recommendation and coverage costs cascade down to low-income families, the gap does not open uniformly. It opens hardest in exactly the communities least able to absorb an outbreak: rural counties with limited clinical infrastructure, low-income households where a single unexpected medical expense disrupts everything else, communities where misinformation has been seeded by people with media platforms and no personal exposure to the consequences. Those are where the unvaccinated pockets form. Those are where outbreaks begin. This is not a projection. It is the observed pattern from every major domestic outbreak of the last decade.

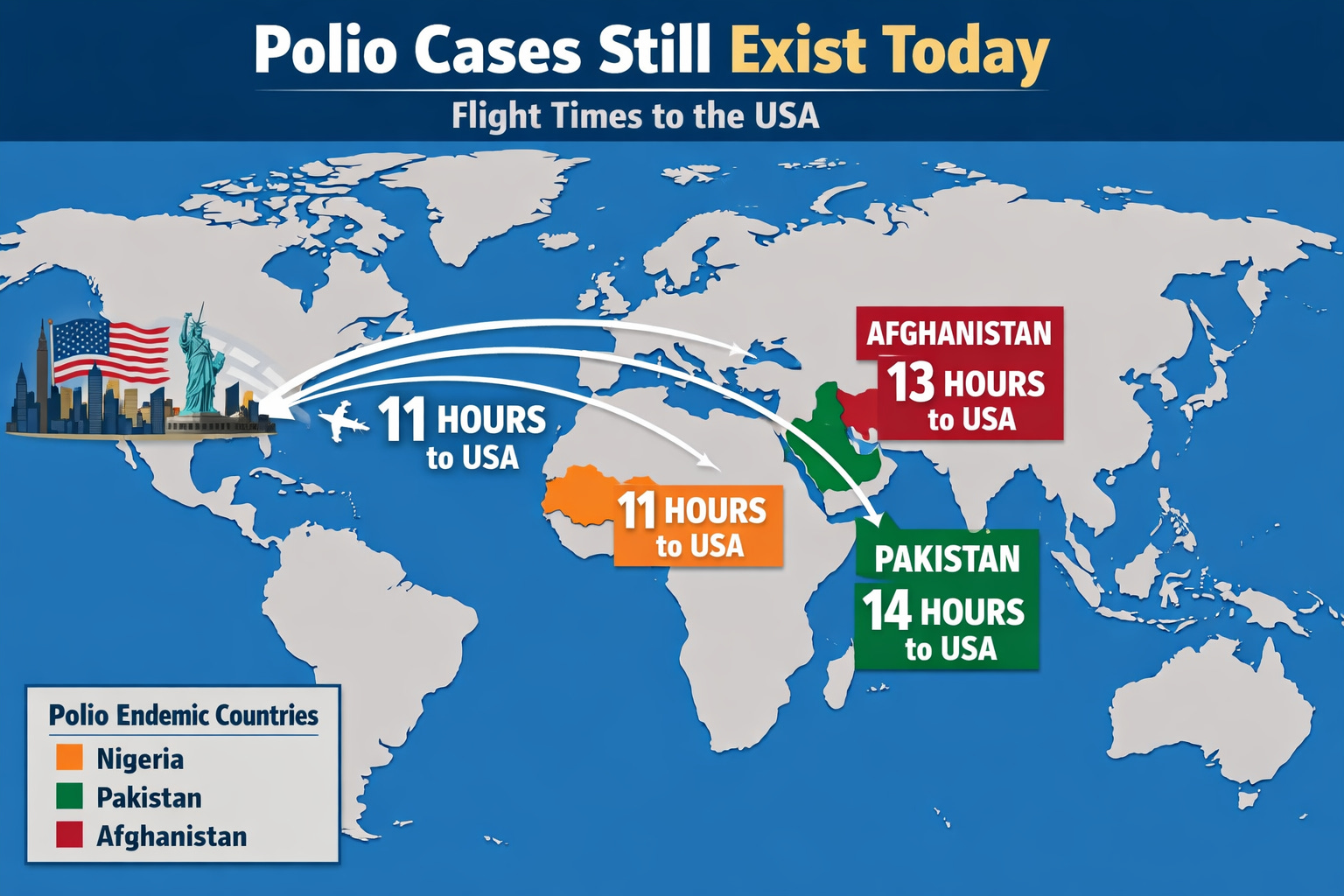
Polio is not a historical curiosity. Wild poliovirus type 1 remains endemic in Pakistan and Afghanistan. Pakistan recorded 99 confirmed cases in 2024, a twelvefold increase from the prior year. Afghanistan reported a fourfold increase over the same period. The World Health Organization has maintained a Public Health Emergency of International Concern for poliovirus without interruption since 2014. Vaccine-derived poliovirus, strains that mutated back toward virulence after circulating in under-immunized populations, has produced outbreaks across Nigeria, Chad, the Democratic Republic of Congo, Somalia, Yemen, Ethiopia, Indonesia, Algeria, Guinea, and Papua New Guinea. In early 2025, a Nigerian-origin poliovirus strain turned up in wastewater samples across 16 cities in five European countries. In August 2025, the CDC issued a Level 2 travel advisory covering poliovirus exposure risk in 41 countries. The virus does not observe borders or respect the preferences of people who have decided it no longer poses a threat. In 2022, it paralyzed an unvaccinated young adult in Rockland County, New York. Wastewater surveillance identified the same strain in surrounding counties, indicating that the one visible paralysis case was the surface of a much larger iceberg of silent infection moving through an under-vaccinated community. The paralysis rate for that circulating strain is roughly one in 2,000 infections. The math is straightforward and the math is brutal.
The consensus that vaccines are safe and effective is not the product of regulatory capture or industry corruption. It is the product of randomized controlled trials, post-market surveillance data covering hundreds of millions of doses, and independent replication across research systems in dozens of countries with no shared financial interest in the outcome. To believe it is fraudulent, you must believe that researchers in the United States, Europe, Japan, Australia, Canada, and across the developing world, operating under different regulatory frameworks, funded through different channels, publishing in competing journals with competing editorial standards, have all independently arrived at the same false conclusion. You must further believe that an environmental lawyer and an evangelical cardiologist have identified what all of them missed. That level of epistemic self-regard is not skepticism. It is a faith position, and it is no more amenable to evidence than the one Milhoan described when he explained that his higher authority is God.
These men are cruel and they are self-serving, and the consequences of that cruelty are not waiting on the horizon — they are already here. Whooping cough is back. Measles is back. Children are sick right now from diseases that were effectively beaten, defeated by the same public health infrastructure these men have spent years undermining for audiences, for donations, for relevance. Polio is not back yet. That word — yet — is doing a lot of work. The conditions for its return are being actively assembled by people who will not be the ones watching their children lose the use of their legs. What is being built here is not a policy disagreement. It is a machine for transferring suffering onto the most vulnerable people in the country.
*I’ve written extensively on RFK Jr. - You can find those articles in the archives.

Why Your Subscription Matters
Independent journalism answers to readers—not advertisers, corporations, or access-hungry editors. No story gets killed because it upsets a sponsor. No punch gets pulled because someone important made a phone call.
Your support makes possible sharp commentary, fearless satire, and reporting that follows the story wherever it leads. In an era of manufactured narratives and algorithmic blandness, that independence isn’t a luxury—it’s a necessity.
Subscribe to The Powell House Press. Or settle for content that tells you what someone else wants you to hear.
©2026 The Powell House Press | josh@thepowellhousepress.com
Let's just go back to the dark ages. If you are unfortunate enough to get a disease, then you must have a demon in you that must be exorcised by a trial by water of fire.