

The Freezer Full of Roadkill and Empty Policy
We know a worm lurks in RFK Jr.’s brain, but what about his freezer?

Somewhere on Interstate 684, on a November afternoon in 2001, a man pulled his minivan onto the shoulder, left his children waiting in their seats, and knelt beside a dead raccoon to cut off its penis. He wanted, he later wrote, to study it. The scene comes from his own diary, published this spring in Isabel Vincent’s biography RFK Jr.: The Fall and Rise, drawn from journal entries he made between 1999 and 2001. He has neither confirmed nor denied it. The raccoon, we can assume, offered no comment either.
This would be merely one of the great cocktail-party anecdotes of the age (alongside the roadkill bear cub he left in Central Park in 2014 and the whale head his daughter says he once strapped to the roof of the family minivan) were it not for the small matter of the man’s current job. Robert F. Kennedy Jr. runs the Department of Health and Human Services. He collects roadkill; he now also collects the fate of the nation’s vaccine policy. When Jesse Watters asked him on Fox in June whether he would “leave the raccoons alone,” Kennedy replied, “Yes. For the moment.”
Hold that image, because it is almost too perfect. I-684 runs through Westchester County, which is to say straight through the heart of the American Northeast’s raccoon-rabies belt, the very corridor where the virus has been enzootic since the 1970s. The raccoon is not an incidental prop in the rabies story. It is a principal player. And the dead one on the shoulder of the highway was, in the crispest epidemiological sense, a potential vector: rabies can pass from a carcass to a person through saliva or neural tissue meeting broken skin, which is precisely the sort of contact a roadside dissection invites. The man dismantling the public-health apparatus that keeps rabies at bay was, per his own account, performing amateur necropsies on one of its favorite hosts. You could not make it up. You would not dare.
The Disease That Waits
Rabies occupies a strange and privileged corner of American medicine: one of the deadliest viruses known, effectively 100 percent fatal once symptoms bloom, and yet it kills only a handful of Americans a year. That gap is not luck. It is the dividend of a century of unglamorous work: animal vaccination, wildlife surveillance, and a treatment protocol that succeeds nearly every time it is deployed on schedule. It is, in other words, exactly the kind of invisible machinery that a culture takes for granted until someone starts pulling out the wiring to see what happens.
The numbers are almost soothing. Fewer than ten Americans die of rabies each year, down from the several hundred who died annually before 1960. From 2015 to 2024, seventeen human cases were recorded, two of them contracted abroad. Set that against the churn beneath it: roughly 1.4 million Americans seek medical care after animal contact each year, and about 100,000 receive rabies shots afterward. The distance between 100,000 treatments and fewer than ten deaths is the whole story of rabies in America, told in a single ratio.
But the disease has not gone anywhere. It is merely waiting, permanently established in the wild. It lives in every state but Hawaii. Some 4,000 rabid animals turn up each year, more than 90 percent of them wildlife. Three of every four Americans live somewhere raccoons, skunks, or foxes carry it.
Any mammal can catch rabies, but a small cast sustains it: bats, raccoons, skunks, foxes. This is a plot twist from the mid-century, when the villain was the family dog. Strict pet-vaccination laws eliminated the canine strain, and the United States has been free of dog rabies since 2007. An achievement, incidentally, of the same regulatory state now being audited for sport.
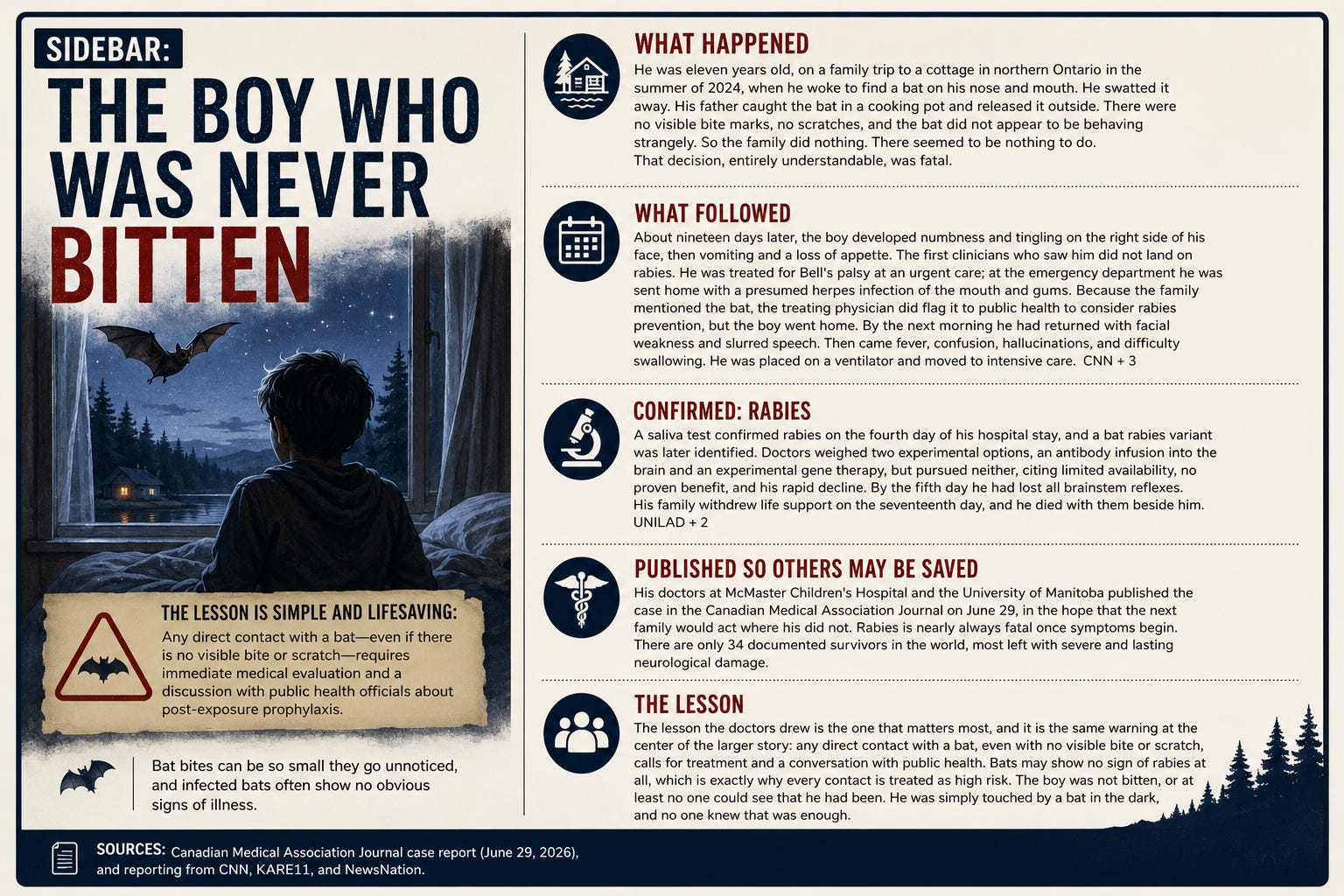
Today the bat is the leading man. Of the 42 rabies cases Americans acquired at home between 2000 and 2024, bats caused 35, or 83 percent. The reason is horribly banal. Bat teeth are small; their bites leave marks that a person can miss entirely, a nip in the night dismissed by morning. The silver-haired bat and the tricolored bat account for roughly 60 percent of the identified infections, two unassuming creatures doing outsized damage.
The 2025 deaths sketch the range. One was a child bitten by a dog in India who died after reaching the United States. The other was an organ-transplant recipient who received a kidney from a donor exposed to a rabid skunk in Idaho; the donor never sought care, died without the classic symptoms, and was never flagged. Rabies, it turns out, can arrive by highway, by airport, by operating table.
The Shot Before the Bite
Here is the part the anti-vaccine set would prefer you forget: there is a rabies vaccine, and you can take it before anything ever bites you. Preexposure prophylaxis, in the jargon. It is not for everyone. It is aimed at the exposed professions (veterinarians, animal-control officers, wildlife biologists, lab workers, spelunkers, anyone who handles bats or, one supposes, harvests raccoons at the roadside). Since 2022 the regimen is mercifully short: two doses, day zero and day seven, good for up to three years, with a titer check or a booster after that.
And then there are travelers. Rabies kills an estimated 59,000 people a year worldwide, the deaths clustering in Asia, at about 60 percent, and Africa, at about 36 percent. In much of India, Bangladesh, the Philippines, and across Nigeria, Kenya, and Tanzania, the arithmetic is grim and identical: too many stray dogs, too little immediate care. Dog bites cause roughly 99 percent of human rabies cases globally, the very scourge America engineered away at home. The CDC advises travelers bound for these places, especially the ones going far from a good hospital, to consider the vaccine first. The backpacker loose in rural India for a season is a candidate; the executive doing two nights in a five-star tower is not.
The case for the pre-trip shot is really a case about what happens after the bite. Rabies immune globulin, the thing that protects an unvaccinated person immediately, is expensive and frequently nowhere to be found in exactly the countries where you would need it most. Get bitten without it and your holiday becomes a medical evacuation. Get vaccinated beforehand and the whole crisis shrinks: you skip the immune globulin entirely and need only two follow-up doses. It does not spare you the trip to a clinic. It spares you the panic. Travel-medicine specialists suggest starting the series four to six weeks before you fly.
There is no cure once rabies takes hold. Everything is prevention, delivered after exposure but before symptoms, and it is called postexposure prophylaxis. It is widely available in America and it very nearly always works.
For the never-vaccinated, it comes in three parts. First, wash the wound, thoroughly, with soap and water, and a virucidal like povidone-iodine if you have it. Second, human rabies immune globulin, infiltrated around the wound where possible to neutralize the virus on the spot. Third, the vaccine series: a dose at the first visit, then days three, seven, and fourteen (a fifth dose on day twenty-eight for the immunocompromised). The globulin guards the opening while the vaccine takes seven to ten days to raise the body’s own defenses. The already-vaccinated need less: two doses, three days apart, no globulin.
Now, the timing, which is where folklore does the most damage. The first dose should go in as soon as possible. That is the rule. But there is no magic cutoff after which treatment becomes pointless; the vaccine-and-globulin combination is recommended regardless of how much time has passed since exposure, so long as symptoms have not begun. The person who realizes only weeks later what that fluttering thing in the bedroom might have been should still go. The one firm deadline governs the immune globulin, not the vaccine: it must be given within seven days of the first shot, after which the vaccine has taken over and the globulin adds nothing.
The real deadline is not on any chart. It is biological. Rabies is nearly always fatal if treatment does not begin before symptoms start; once the virus reaches the brain, nothing helps. Every recent American death is a variation on the same sentence. The two people who died in 2024, in Minnesota and California, both had a recognized bat encounter, both told no one, both waited. The virus does not negotiate. It simply keeps its appointment.
The Wall, and the People Pulling Bricks
Which returns us, unavoidably, to the man with the freezer full of roadkill. The thing about rabies is that its rarity is entirely manufactured, a public good built and maintained by the institutions now in his charge. And the maintenance is faltering. As HHS secretary, Kennedy, a lifelong vaccine skeptic, dismissed all seventeen members of the CDC’s vaccine advisory committee and installed his own, several with track records of overstating vaccine harms. A federal judge in Boston found the panel’s decisions arbitrary and capricious and put them on hold; the same judge called most of Kennedy’s appointees “distinctly unqualified.” The department rewrote the childhood vaccine schedule to resemble Denmark’s, cutting it from eighteen diseases to eleven, and rolled back the decades-old recommendation that newborns receive a hepatitis B shot within a day of birth. It wound down mRNA vaccine development and cancelled nearly $500 million in funding.
None of these moves is about rabies, specifically. That is the point. Rabies is the canary, not the coal. A society that keeps a nearly universally fatal virus down to single-digit deaths does it through exactly the machinery being dismantled: the surveillance, the vaccine advisory science, the patient public education that teaches a person to take a bat bite seriously. Weaken the wall in general and you do not get to choose which disease walks through the gap. The genius of rabies control was that most Americans never had to think about rabies at all. The tragedy, if it comes, will be that they will have to start.
For the moment, the secretary assures us, the raccoons are safe. The rest of us he did not mention.
Sources: CDC National Rabies Surveillance data, clinical guidance, MMWR reports, and the Yellow Book; ACIP pre- and post-exposure recommendations; reporting from CNN, NBC News, PBS/AP, NPR, STAT, People, and NewsNation; and Isabel Vincent, “RFK Jr.: The Fall and Rise.”
